DC Mask Usage--Uncaptioned version
Anonymous
|
Anonymous
|
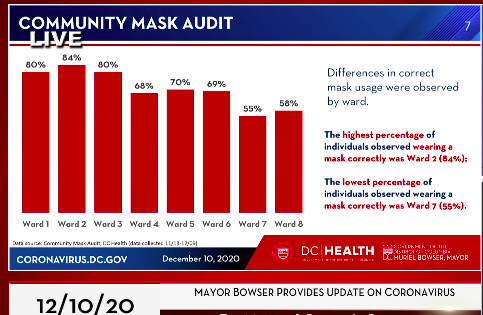
Ward 2, leading the city. No surprise.
Ward 8, worst compliance of all. No surprise there either. |
Anonymous
And why is that? Signed, Ward 8 resident of 25 years. |
Anonymous
|
Was this based on survey, observation or what?
Interesting—I’m in Ward 4, but compliance seems pretty high walking around my neighborhood. |
Anonymous
|
I have a hypothesis that is not directly linked to race and SES. Many of my Ward 4 neighbors are essential or had jobs that could not go virtual. They have high rates of potential exposure working at daycares, healthcare settings, home repair, etc. When the actual risk is constant, it is easier to mentally fatigue: No one can be ever-vigilant. It may also be easier to reason “I did not get sick at work where the risk is higher. Going to the park or grocery is not going to be where I fall ill.”
My other hypothesis has to do with age. Wards 4 and 8 have a high population of kids and teens relative to other wards. Young people are always poor at gauging risk. Further compounding the problem, there has been a lot of messaging in the pandemic about how young people don’t get as sick and how schools should be safe. It’s easier to rationalize not wearing an uncomfortable mask when this is what you’ve heard. |
Anonymous
Yeah, I'm curious about the methodology there, but your explanation makes sense, especially wrt teenagers, who are notoriously bad at evaluating risk. And it also makes sense that people who have to wear masks MORE because of their jobs might slack off sometimes. It's easy to wear a mask when I'm outside for a couple hours a day, max. Maybe harder to do so if I have to wear it 8+ hours. Plus, depending on when they did the observation, a lot of Ward 4/7/8 residents might well be working in another ward, and wearing a mask at work. I'd also note that mask compliance appears to be above 50 percent everywhere, which means the majority of people *are* wearing masks. |
Anonymous
Young people are at very low risk from this virus. A teenager who doesn’t wear a mask is assessing their risk correctly. |
Anonymous
Assessing risk well also includes risk of infecting others and therefore includes risk to others. I don't know any kids who want to infect their parents or grandparents, but a poor risk assessor might not take that into account. |
Anonymous
+1 The evidence is that teenagers spread COVID as effectively as young adults. Teens might be assessing their own risk reasonably well, but not considering that they could be the vector for infecting a parent, grandparent, or other vulnerable family member. |
Anonymous
|
Without knowing what “were observed” means, it’s hard to know how to understand the data. Who did the observing — and how? I think several PPs have made plausible inferences, but without knowing more about even the basics of how this was carried out, I have no conclusions to even jump to.
Who did the observations? Where were they done? Were the numbers in each cohorts similar? Or, as has already been discussed, the distributions of age and gender? Were the people observed actively working vs living in the communities in which they were observed? Does it matter? Is the goal of publishing this to increase “correct mask usage”? How was “correct” assessed? So many questions 🤔 tldr: Eh. |
Anonymous
If you’ve really lived in Ward 8 for 25 years, you wouldn’t be asking this question. |
Anonymous
Actually, Ward 7 has the worst compliance. Says so right on the graphic. |
Anonymous
Oh c'mon racist you can do better than that tired old trope. |
Anonymous
So triggered. 
|
Anonymous
| Could this partially explain the disproportionate impact the disease is having on AA? Or are we not allowed to talk about that? |